Normal aging is associated with multiple changes in pharmacokinetic processes, progressive decline in organ function, multiple comorbidities, and a greater risk of polypharmacy. In this article, we explore the impact of the aging process on pharmacokinetics and the implications of these changes on medication management in elderly populations.
Age-Related Changes in Drug Absorption
With age comes changes in the digestive system, such as delays in gastric emptying, decreased gastric acidity, decreased intestinal motility, and decreased splanchnic blood flow.1 Despite these physiological changes, drug absorption remains relatively unchanged in healthy older adults.2
However, certain diseases (e.g., atrophic gastritis) and drugs that are commonly used in elderly populations (e.g., antacids, proton pump inhibitors, bowel medications) can increase gastric pH, reduce absorption, and consequently delay the onset of action of other medications.3-6
Age-Related Changes in Drug Distribution
Aging is associated with relative increases in body fat due to decreased lean body mass and total body water.7 Greater body fat increases the volume of distribution (Vd) of highly lipophilic drugs (e.g., diazepam, chlordiazepoxide), leading to higher elimination half-lives (T1/2).8,9 Additionally, because lipophilic drugs are quickly taken up by fat stores, repeated dosing can result in significant accumulation in fat, resulting in erratic release and changing serum levels as time progresses.10,11
In contrast, water-soluble drugs (e.g., digoxin, lithium, aminoglycosides) will have a smaller Vd as relative body fat increases, leading to more circulating drug and higher plasma concentrations.10,12
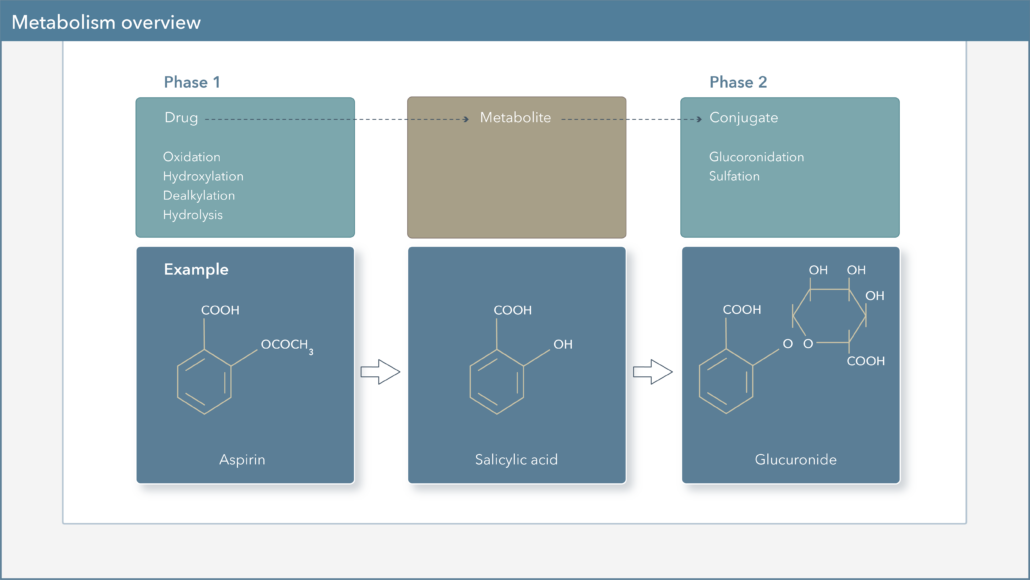
Age-Related Changes in Drug Metabolism
Aging may lead to changes in the function of various CYP450 enzymes important in Phase I oxidation reactions. Although data on these changes are inconsistent, literature supports a decrease in the function of CYP1A2 and CYP2C19, while CYP3A4, CYP2C9, and CYP2D6 metabolic rates may remain unchanged.13 Additionally, Phase II glucuronidation reactions are generally unaffected by normal aging; as such, UGT enzyme function may not be changed by the aging process.14,15 However, it is essential to recognize that the activities of both CYP450 and UGT enzymes may also be influenced by drug-drug interactions, which can lead to alterations in overall drug exposure and clearance of substrates of these metabolic pathways. Furthermore, decreased hepatic blood flow in the elderly population can reduce the metabolism and clearance of drugs with high extraction ratios, such as morphine, verapamil, and lidocaine.14
Drug-Drug Interactions in the Elderly Population
A patient taking five to nine medications has a 50% probability of a drug-drug interaction and approximately 44% of men and 57% of women older than 65 years take five or more nonprescription and/or prescription medications per week.24
In addition to the impact CYP450 enzymes have on the metabolism of individual drugs, this enzyme family is also an important consideration in drug-drug interactions.16 Various medications can act as inhibitors or inducers of CYP450 enzymes, leading to alterations in the activity of these enzymes and their ability to metabolize other medications. This, in turn, can lead to increased or decreased concentrations of other medications, which may be associated with toxicities or changes in efficacy, respectively.
Age-Related Changes in Drug Excretion
Decreased renal elimination of drugs results in significant pharmacokinetic changes in older populations. Anatomical changes in the renal system, such as loss of glomeruli and renal mass, can lead to reduced glomerular filtration rate (GFR).17 GFR declines progressively with age, even in patients without renal disease. Accelerated decline in GFR tends to manifest after age 65-70, although GFR typically begins to decline at 30-40 years of age.18 For example, in healthy kidney donors, it was noted that GFR declined at a rate of 6.3 ml/min/1.73 m2 with each decade.19
Older adults tend to have less muscle mass and are typically less physically active, leading to lower creatinine production and a calculated creatinine clearance that may overestimate true clearance.20 Drugs that are mainly renally excreted (e.g., aminoglycosides, lithium, and digoxin) may result in toxicity in older patients.21-23
In Conclusion
It is estimated that 35% of ambulatory older adults experience an adverse drug reaction each year, and 29% of these reactions require hospitalization.24 It is important to consider the impact of the aging process on pharmacokinetics when prescribing for elderly individuals. Greater volume of distribution, declining CYP450 function, and reduced renal clearance are just some of the age-related changes in pharmacokinetics that contribute to the heightened risk of adverse events and drug toxicity in older populations.
It is essential to recognize that polypharmacy is especially common in elderly patients and that the activities of drug metabolizing enzymes are influenced by drug-drug interactions. Knowing there is an even greater drug interaction risk for elderly patients, Genomind provides clinicians with access to Genomind’s Precision Medicine Software.
Are You Ready to Upgrade Your Practice with Genomind?
Genomind’s pharmacogenetic testing is the most advanced and comprehensive mental health pharmacogenetic test available. Get access to 26 genes related to mental health, 130+ medications, 10+ conditions, state-of-the-art tools, and 360 degrees of support – register today.
References
- Kekki M, Samloff IM, Ihamäki T, Varis K, Siurala M. Age- and sex-related behaviour of gastric acid secretion at the population level. Scand J Gastroenterol. 1982 Sep;17(6):737-43.
- Greenblatt DJ, Sellers EM, Shader RI. Drug therapy: drug disposition in old age. N Engl J Med. 1982 May 6;306(18):1081-8.
- Cavalcoli F, Zilli A, Conte D, Massironi S. Micronutrient deficiencies in patients with chronic atrophic autoimmune gastritis: A review. World J Gastroenterol. 2017 Jan 28;23(4):563-572.
- Kinoshita Y, Ishimura N, Ishihara S. Advantages and Disadvantages of Long-term Proton Pump Inhibitor Use. J Neurogastroenterol Motil. 2018 Apr 30;24(2):182-196.
- Romankiewicz JA. Effects of antacids on gastrointestinal absorption of drugs. Prim Care. 1976 Sep;3(3):537-50.
- Patel D, Bertz R, Ren S, Boulton DW, Någård M. A Systematic Review of Gastric Acid-Reducing Agent-Mediated Drug-Drug Interactions with Orally Administered Medications. Clin Pharmacokinet. 2020 Apr;59(4):447-462.
- Fülöp T Jr, Wórum I, Csongor J, Fóris G, Leövey A. Body composition in elderly people. I. Determination of body composition by multiisotope method and the elimination kinetics of these isotopes in healthy elderly subjects. Gerontology. 1985;31(1):6-14.
- Greenblatt DJ, Allen MD, Shader RI. Toxicity of high-dose flurazepam in the elderly. Clin Pharmacol Ther. 1977;21:355 -61.
- Turnheim, K., 1998. Drug dosage in the elderly. Is it rational? Drugs Aging 13, 357–379.
- Shi S, Klotz U. Age-related changes in pharmacokinetics. Curr Drug Metab. 2011 Sep;12(7):601-10.
- Bruno CD, Harmatz JS, Duan SX, Zhang Q, Chow CR, Greenblatt DJ. Effect of lipophilicity on drug distribution and elimination: Influence of obesity. Br J Clin Pharmacol. 2021 Jan 15.
- Thompson TL 2nd, Moran MG, Nies AS. Drug therapy: Psychotropic drug use in the elderly (first of two parts). N Engl J Med. 1983 Jan 20;308(3):134-8.
- Wauthier V, Verbeeck RK, Buc Calderon P. The effect of aging on cytochrome P450 enzymes: consequences for drug biotransformation in the eldelry. Curr Med Chem 2007;14(7):745-757.
- Le Couteur DG, McLean AJ. The aging liver. Drug clearance and an oxygen diffusion barrier hypothesis. Clin Pharmacokinet. 1998 May;34(5):359-73.
- Klotz, U. Effect of aging on the pharmacokinetics of gastrointestinal drugs. In: Pilotti A, Malferthheiner P, Holt PR(eds.), Aging and the Gastrointestinal Tract. Interdisciplinary Topics in Gerontology. Basel, Switzerland: Karger, 2003; Vol. 32, pp. 28–39.
- Flockhart DA. P450 Drug interaction table: abbreviated “clinically relevant” table. https://medicine.iupui.edu/clinpharm/ddis/ClinicalTable.aspx. Accessed June 3, 2021.
- Clark B. Biology of renal aging in humans. Adv Ren Replace Ther. 2000 Jan;7(1):11-21.
- Macias-Nunez J-F, Lopez-Novoa JM. Physiology of the Healthy Aging Kidney. In: Oreopoulos DM, Cameron JS, Macias Nunez JF, editors. Aging Kidney in Health and Disease. New York: Springer; 2008. pp. 93–112.
- Rule AD, Amer H, Cornell LD, Taler SJ, Cosio FG, Kremers WK, Textor SC, Stegall MD. The association between age and nephrosclerosis on renal biopsy among healthy adults. Ann Intern Med. 2010 May 4;152(9):561-7.
- Raman M, Middleton RJ, Kalra PA, Green D. Estimating renal function in old people: an in-depth review. Int Urol Nephrol. 2017 Nov;49(11):1979-1988.
- Mörike K, Schwab M, Klotz U. Use of aminoglycosides in elderly patients. Pharmacokinetic and clinical considerations. Drugs Aging. 1997 Apr;10(4):259-77.
- Sproule BA, Hardy BG, Shulman KI. Differential pharmacokinetics of lithium in elderly patients. Drugs Aging. 2000 Mar;16(3):165-77.
- Hanratty CG, McGlinchey P, Johnston GD, Passmore AP. Differential pharmacokinetics of digoxin in elderly patients. Drugs Aging. 2000 Nov;17(5):353-62.
- Saljoughian M. Polypharmacy and Drug Adherence in Elderly Patients. U.S Pharm. 2019 July;44(7): 33-36.